山东大学学报 (医学版) ›› 2022, Vol. 60 ›› Issue (11): 44-53.doi: 10.6040/j.issn.1671-7554.0.2022.0960
• 胸外科肺癌、食管癌微创诊治和加速康复专题 • 上一篇 下一篇
彭岳1,2,刘雷1,3,李原1,别凤龙1,周博伦1,李润泽1,冀瑛2,白广宇1,谭锋维1,高禹舜1,牟巨伟1,薛奇1,邱斌1,*( ),高树庚1,*()
),高树庚1,*()
Yue PENG1,2,Lei LIU1,3,Yuan LI1,Fenglong BIE1,Bolun ZHOU1,Runze LI1,Ying JI2,Guangyu BAI1,Fengwei TAN1,Yushun GAO1,Juwei MU1,Qi XUE1,Bin QIU1,*(),Shugeng GAO1,*()
摘要:
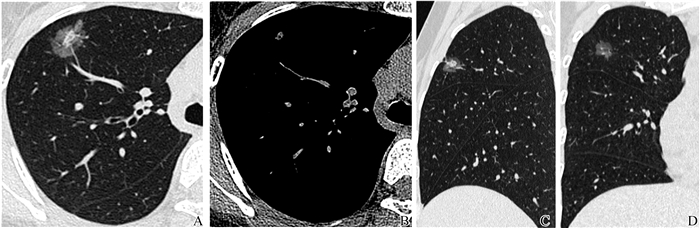
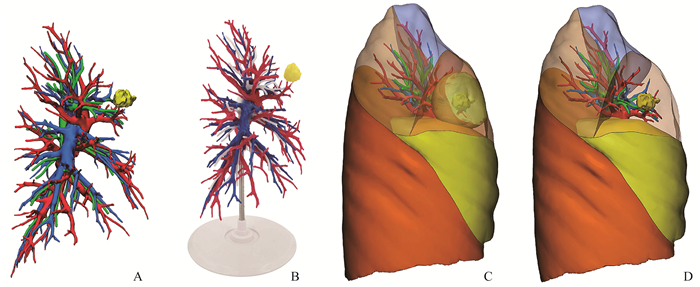
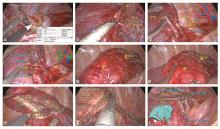
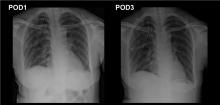
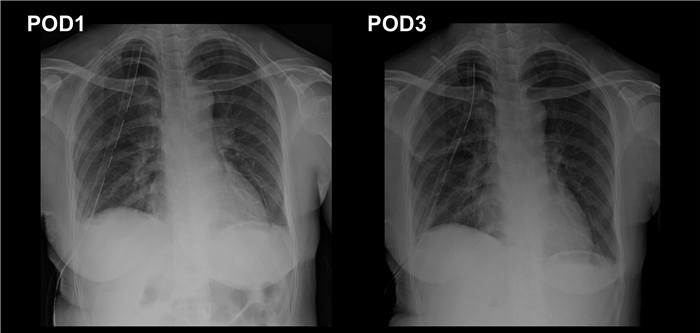
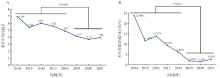
目的: 总结分析解剖性部分肺叶切除术(APL)以及围术期加速康复外科(ERAS)的统筹应用经验,以期为肺癌外科微创治疗的综合管理提供临床参考与理论支持。方法: 回顾性分析中国医学科学院肿瘤医院胸外科肺癌数据库2013年11月1日至2021年10月31日接受APL手术的6 449例患者的临床病理学资料以及围手术期数据,包括性别、年龄、吸烟史、手术方式、病理、术后住院日等指标。以2014—2018年作为经验积累阶段,2019—2021年作为技术成熟阶段。比较两阶段在手术量、良性结节占比、术后平均住院日、术后住院日超7 d的差异。结果: 纳入患者6 449例,其中男2 094例,女4 355例。分期完成两侧肺部手术88台,同期完成双侧手术8台,共完成APL手术6 493台。技术成熟阶段较经验积累阶段的年度月均手术量增加、良性结节占比减少、术后平均住院日缩短、术后住院日超7 d占比减少(P<0.05)。通过结合ERAS理念优化本中心APL围术期管理细节,成功使得患者术后平均住院日从6.98 d显著降至3.96 d。术后住院日超7 d患者占比由23.80%降至2.87%,多因素Logistic回归分析结果显示性别、年龄、手术术式、手术阶段是APL术后住院日超7 d的独立危险因素。结论: ERAS能够优化APL围术期管理流程,加速患者术后康复。而APL手术可以在保证肿瘤学原则的前提下,为患者保留更多的健康肺组织,实现手术切除范围、手术创伤的最小化,为ERAS理念能够更好地在肺癌根治手术中应用推广提供了必要的临床实践基础。
中图分类号:
| 1 | Kehlet H , Mogensen T . Hospital stay of 2 days after open sigmoidectomy with a multimodal rehabilitation programme[J]. Br J Surg, 1999, 86 (2): 227- 230. |
| 2 |
Miller TE , Thacker JK , White WD , et al. Reduced length of hospital stay in colorectal surgery after implementation of an enhanced recovery protocol[J]. Anesth Analg, 2014, 118 (5): 1052- 1061.
doi: 10.1213/ANE.0000000000000206 |
| 3 |
Kehlet H . Fast-track colorectal surgery[J]. Lancet, 2008, 371 (9615): 791- 793.
doi: 10.1016/S0140-6736(08)60357-8 |
| 4 |
Ljungqvist O , Scott M , Fearon KC . Enhanced recovery after surgery: a review[J]. JAMA Surg, 2017, 152 (3): 292- 298.
doi: 10.1001/jamasurg.2016.4952 |
| 5 |
Duan L , Jiang G , Yang Y . One hundred and fifty-six cases of anatomical pulmonary segmentectomy by uniportal video-assisted thoracic surgery: a 2-year learning experience[J]. Eur J Cardiothorac Surg, 2018, 54 (4): 677- 682.
doi: 10.1093/ejcts/ezy142 |
| 6 | Hernandez-Arenas LA , Purmessur RD , Gonzalez-Rivas D . Uniportal video-assisted thoracoscopic segmentectomy[J]. J Thorac Dis, 2018, 10 (suppl 10): S1205- S1214. |
| 7 |
Bertolaccini L , Batirel H , Brunelli A , et al. Uniportal video-assisted thoracic surgery lobectomy: a consensus report from the Uniportal VATS Interest Group (UVIG) of the European Society of Thoracic Surgeons (ESTS)[J]. Eur J Cardiothorac Surg, 2019, 56 (2): 224- 229.
doi: 10.1093/ejcts/ezz133 |
| 8 |
Han D , Cao Y , Wu H , et al. Uniportal video-assisted thoracic surgery for the treatment of lung cancer: a consensus report from Chinese Society for Thoracic and Cardiovascular Surgery (CSTCVS) and Chinese Association of Thoracic Surgeons (CATS)[J]. Transl Lung Cancer Res, 2020, 9 (4): 971- 987.
doi: 10.21037/tlcr-20-576 |
| 9 |
邱斌, 冀瑛, 张帆, 等. 解剖性部分肺叶切除术治疗3 336例肺结节患者的疗效[J]. 中华肿瘤杂志, 2021, 43 (1): 137- 142.
doi: 10.3760/cma.j.cn112152-20201014-00900 |
|
QIU Bin , JI Ying , ZHANG Fan , et al. Anatomical partial lobectomy for the treatment of 3, 336 cases of patients with lung nodule[J]. Chinese Journal of Oncology, 2021, 43 (1): 137- 142.
doi: 10.3760/cma.j.cn112152-20201014-00900 |
|
| 10 |
Qiu B , Ji Y , Zhang F , et al. Outcomes and experience of anatomical partial lobectomy[J]. J Thorac Cardiovasc Surg, 2022, 164 (3): 637- 647.
doi: 10.1016/j.jtcvs.2021.11.044 |
| 11 |
邱斌, 冀瑛, 白广宇, 等. 解剖性部分肺叶切除术治疗早期肺癌: 实践与发展[J]. 中华胸部外科电子杂志, 2020, 7 (4): 240- 246.
doi: 10.3877/cma.j.issn.2095-8773.2020.04.07 |
|
QIU Bin , JI Ying , BAI Guangyu , et al. Clinical practice and development on anatomic partial lobectomy for early-stage lung cancer[J]. Chinese Journal of Thoracic Surgery (Electronic Edition), 2020, 7 (4): 240- 246.
doi: 10.3877/cma.j.issn.2095-8773.2020.04.07 |
|
| 12 |
Qiu B , Ji Y , He H , et al. Three-dimensional reconstruction/personalized three-dimensional printed model for thoracoscopic anatomical partial-lobectomy in stage I lung cancer: a retrospective study[J]. Transl Lung Cancer Res, 2020, 9 (4): 1235- 1246.
doi: 10.21037/tlcr-20-571 |
| 13 |
Oizumi H , Endoh M , Takeda S , et al. Anatomical lung segmentectomy simulated by computed tomographic angiography[J]. Ann Thorac Surg, 2010, 90 (4): 1382- 1383.
doi: 10.1016/j.athoracsur.2009.11.062 |
| 14 |
Oizumi H , Kanauchi N , Kato H , et al. Anatomic thoracoscopic pulmonary segmentectomy under 3-dimensional multidetector computed tomography simulation: a report of 52 consecutive cases[J]. J Thorac Cardiovasc Surg, 2011, 141 (3): 678- 682.
doi: 10.1016/j.jtcvs.2010.08.027 |
| 15 |
车国卫. 加速康复外科: 临床应用加减之间?[J]. 中国肺癌杂志, 2019, 22 (11): 681- 686.
doi: 10.3779/j.issn.1009-3419.2019.11.01 |
|
CHE Guowei . Proper selection of enhanced recovery after surgery programs between the medical service and medical intervence-is it time to do?[J]. Chinese Journal of Lung Cancer, 2019, 22 (11): 681- 686.
doi: 10.3779/j.issn.1009-3419.2019.11.01 |
|
| 16 | 支修益, 刘伦旭, 中国胸外科围手术期气道管理指南版编写委员会. 中国胸外科围手术期气道管理指南(2020版)[J]. 中国胸心血管外科临床杂志, 2021, 28(3): 251-262. |
| ZHI Xiuyi, LIU Lunxu. Chinese guidelines for perioperative airway management in thoracic surgery (2020 edition)[J]. Chinese Journal of Clinical Thoracic and Cardiovascular Surgery, 2021, 28(3): 251-262. | |
| 17 |
Mills E , Eyawo O , Lockhart I , et al. Smoking cessation reduces postoperative complications: a systematic review and meta-analysis[J]. Am J Med, 2011, 124 (2): 144- 154.
doi: 10.1016/j.amjmed.2010.09.013 |
| 18 |
Berger M , Schenning KJ , Brown CH , et al. Best practices for postoperative brain health: recommendations from the fifth international perioperative neurotoxicity working group[J]. Anesth Analg, 2018, 127 (6): 1406- 1413.
doi: 10.1213/ANE.0000000000003841 |
| 19 |
Tiwary N , Treggiari MM , Yanez ND , et al. Agreement between the mini-cog in the preoperative clinic and on the day of surgery and association with postanesthesia care unit delirium: a cohort study of cognitive screening in older adults[J]. Anesth Analg, 2021, 132 (4): 1112- 1119.
doi: 10.1213/ANE.0000000000005197 |
| 20 | 刘子嘉, 张路, 刘洪生, 等. 基于加速术后康复的胸外科手术预康复管理专家共识(2022)[J]. 协和医学杂志, 2022, 13 (3): 387- 401. |
| LIU Zijia , ZHANG Lu , LIU Hongsheng , et al. Expert consensus on prehabilitation management for enhanced recovery in patients undergoing thoracic surgery (2022)[J]. Medical Journal of Peking Union Medical College Hospital, 2022, 13 (3): 387- 401. | |
| 21 | Lumb AB . Pre-operative respiratory optimisation: an expert review[J]. Anaesthesia, 2019, 74 (Suppl 1): 43- 48. |
| 22 |
Lai YT , Su JH , Qiu PY , et al. Systematic short-term pulmonary rehabilitation before lung cancer lobectomy: a randomized trial[J]. Interact CardioVasc Thorac Surg, 2017, 25 (3): 476- 483.
doi: 10.1093/icvts/ivx141 |
| 23 |
Licker M , Karenovics W , Diaper J , et al. Short-term preoperative high-intensity interval training in patients awaiting lung cancer surgery: a randomized controlled trial[J]. J Thorac Oncol, 2017, 12 (2): 323- 333.
doi: 10.1016/j.jtho.2016.09.125 |
| 24 |
Baimas-George M , Watson M , Elhage S , et al. Prehabilitation in frail surgical patients: a systematic review[J]. World J Surg, 2020, 44 (11): 3668- 3678.
doi: 10.1007/s00268-020-05658-0 |
| 25 |
Gao K , Yu PM , Su JH , et al. Cardiopulmonary exercise testing screening and pre-operative pulmonary rehabilitation reduce postoperative complications and improve fast-track recovery after lung cancer surgery: a study for 342 cases[J]. Thorac Cancer, 2015, 6 (4): 443- 449.
doi: 10.1111/1759-7714.12199 |
| 26 |
Low DE , Allum W , De Manzoni G , et al. Guidelines for perioperative care in esophagectomy: enhanced recovery after surgery (ERAS?) society recommendations[J]. World J Surg, 2019, 43 (2): 299- 330.
doi: 10.1007/s00268-018-4786-4 |
| 27 |
Zhou D , Deng XF , Liu QX , et al. Single chest tube drainage is superior to double chest tube drainage after lobectomy: a meta-analysis[J]. J Cardiothorac Surg, 2016, 11 (1): 88.
doi: 10.1186/s13019-016-0484-1 |
| 28 |
Kim SS , Khalpey Z , Daugherty SL , et al. Factors in the selection and management of chest tubes after pulmonary lobectomy: results of a national survey of thoracic surgeons[J]. Ann Thorac Surg, 2016, 101 (3): 1082- 1088.
doi: 10.1016/j.athoracsur.2015.09.079 |
| 29 |
Zhang TX , Zhang Y , Liu ZD , et al. The volume threshold of 300 versus 100 ml/day for chest tube removal after pulmonary lobectomy: a meta-analysis[J]. Interact Cardio Vasc Thorac Surg, 2018, 27 (5): 695- 702.
doi: 10.1093/icvts/ivy150 |
| 30 | 张娜, 张欢欢, 李玉善, 等. 加速康复外科理念下肺肿瘤患者术后病房留置尿管危险因素的病例对照研究[J]. 中国胸心血管外科临床杂志, 2021, 28 (7): 821- 825. |
| ZHANG Na , ZHANG Huanhuan , LI Yushan , et al. Risk factors for postoperative retention of urinary catheters in patients with lung tumors under concept of enhanced recovery after surgery: a case-control study[J]. Chinese Journal of Clinical Thoracic and Cardiovascular Surgery, 2021, 28 (7): 821- 825. | |
| 31 |
Brunelli A . Deep vein thrombosis/pulmonary embolism: prophylaxis, diagnosis, and management[J]. Thorac Surg Clin, 2012, 22 (1): 25- 28.
doi: 10.1016/j.thorsurg.2011.08.014 |
| 32 |
姚丽, 郑娥, 杨梅, 等. 基于患者报告结局的胸腔镜肺癌切除术后患者症状调查[J]. 中国胸心血管外科临床杂志, 2022, 1- 6.
doi: 10.7507/1007-4848.202112082 |
|
YAO Li , ZHENG E , YANG Mei , et al. A survey of symptoms after thoracoscopic lung cancer resection based on patient reported outcomes[J]. Chinese Journal of Clinical Thoracic and Cardiovascular Surgery, 2022, 1- 6.
doi: 10.7507/1007-4848.202112082 |
|
| 33 |
Dai W , Feng W , Zhang Y , et al. Patient-reported outcome-based symptom management versus usual care after lung cancer surgery: a multicenter randomized controlled trial[J]. J Clin Oncol, 2022, 40 (9): 988- 996.
doi: 10.1200/JCO.21.01344 |
| 34 | 沈诚, 李珏, 李鹏飞, 等. 加速康复外科评价指标: 病人报告结局在胸外科的临床应用现状与进展[J]. 中国肺癌杂志, 2019, 22 (3): 161- 166. |
| SHEN Cheng , LI Jue , LI Pengfei , et al. Evaluation index of enhanced recovery after surgery: status and progress of patient report outcomes in thoracic surgery[J]. Chinese journal of lung cancer, 2019, 22 (3): 161- 166. | |
| 35 |
Fagundes CP , Shi Q , Vaporciyan AA , et al. Symptom recovery after thoracic surgery: measuring patient-reported outcomes with the MD Anderson Symptom Inventory[J]. J Thorac Cardiovasc Surg, 2015, 150 (3): 613- 619.
doi: 10.1016/j.jtcvs.2015.05.057 |
| 36 | 车国卫. 加速康复外科: 肺癌手术日间化现状与策略[J]. 中国肺癌杂志, 2020, 23 (1): 1- 4. |
| CHE Guowei . Current situation and strategy of day surgery in patients with lung cancer by enhanced recovery after surgery[J]. Chinese journal of lung cancer, 2020, 23 (1): 1- 4. |
| [1] | 韩靖,贾春玲. 肺癌患者胸外手术前治疗牙周基础疾病对预防术后肺炎发生的效果评价[J]. 山东大学学报 (医学版), 2022, 60(9): 113-118. |
| [2] | 高中霞,张铭,樊明德,谭晨阳,王梦迪,王超,樊跃飞,丁守銮,王成伟. 伽玛刀治疗81例肺癌脑转移瘤的疗效及预后因素[J]. 山东大学学报 (医学版), 2022, 60(8): 44-49. |
| [3] | 王福立,孙银萍,秦杰,荣建胜. DC-CIK细胞联合EGFR-TKI治疗35例老年晚期EGFR突变肺癌的效果[J]. 山东大学学报 (医学版), 2022, 60(7): 110-117. |
| [4] | 秦静,杨飞,陈谦,夏涵岱,刘延国,王秀问. 晚期驱动基因阴性、PD-L1表达阴性非鳞非小细胞肺癌一线治疗方案的网状Meta分析[J]. 山东大学学报 (医学版), 2022, 60(7): 74-82. |
| [5] | 陈兆波,方敏,薛浩然,刘春艳. 去泛素化酶USP35促进非小细胞肺癌细胞迁移和侵袭[J]. 山东大学学报 (医学版), 2022, 60(4): 30-37. |
| [6] | 马瑞杰,朱良明,左太阳,李春海,张楠,孙志钢. 微波消融治疗非小细胞肺癌根治术后肺寡转移瘤的预后分析[J]. 山东大学学报 (医学版), 2022, 60(12): 63-68. |
| [7] | 高树庚. 加速康复外科在肺癌围术期管理中的应用[J]. 山东大学学报 (医学版), 2022, 60(11): 1-10. |
| [8] | 韩丁培,严越,曹羽钦,孙昕,胡琰霞,汪敏娴,罗艳,施咏梅,谢青,杭钧彪,李鹤成. 加速康复外科理念在胸外科临床实践指导的瑞金医院专家共识[J]. 山东大学学报 (医学版), 2022, 60(11): 11-16. |
| [9] | 刘会宁,彭军,任迎春,杨光,王文豪,刘金锋,田勍. 34例胸腔镜下肺楔形切除与21例肺段切除对位于肺段P区的ⅠA1期非小细胞肺癌治疗比较[J]. 山东大学学报 (医学版), 2022, 60(11): 38-43. |
| [10] | 孙振国,田辉. 加速康复外科指导下微创食管癌切除术流程优化之齐鲁实践[J]. 山东大学学报 (医学版), 2022, 60(11): 33-37. |
| [11] | 高会江,魏煜程. 微创袖式肺叶切除手术:免疫治疗时代的机遇和挑战[J]. 山东大学学报 (医学版), 2022, 60(11): 23-27. |
| [12] | 车国卫. 加速康复外科需要与时俱进[J]. 山东大学学报 (医学版), 2022, 60(11): 17-22. |
| [13] | 丁子琛,王浩桦,周立雯,丛慧文,李承圣,包绮晗,杨毅,王廉源,王素珍,石福艳. 基于贝叶斯累加回归树模型的非小细胞肺癌患者个性化疗效研究[J]. 山东大学学报 (医学版), 2022, 60(10): 92-98. |
| [14] | 于金明,颜薇薇,陈大卫. 肺癌放射免疫新实践[J]. 山东大学学报 (医学版), 2021, 59(9): 1-8. |
| [15] | 江志伟,王刚. 延迟性术后肠麻痹的概念及防治策略[J]. 山东大学学报 (医学版), 2020, 58(5): 1-5. |
|